EPIDURAL= PERIDURAL= EXTRA-DURAL
In the spine, the epidural space (from Ancient Greek ἐπί, "on, upon" + dura mater also known as "epidural cavity", "extradural space" or "peridural space") is an anatomic space that is the outermost part of the spinal canal.
In humans the epidural space contains lymphatics, spinal nerve roots, loose connective tissue, fatty tissue, small arteries, and a network of internal vertebral venous plexuses.
In humans[edit]The upper limit of the epidural space is the foramen magnum, which is the point where the spine meets the base of the skull. The lower limit is at the tip of the sacrum, at the sacrococcygeal membrane.
In the head, the epidural space is known as a potential space. In rare circumstances, a torn artery (e.g. the middle meningeal artery) may cause bleeding which is sufficient to create epidural space; this is an epidural hematoma.
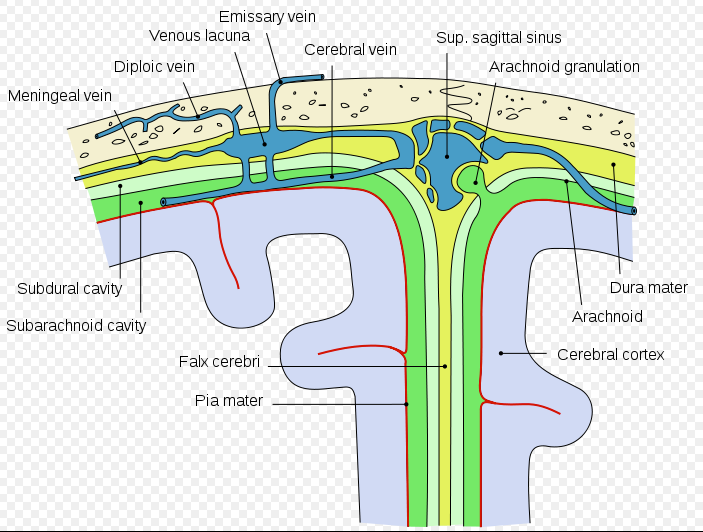
The space between the dura and the arachnoid (in both head and spine), the subdural space, is also a potential space. Bleeding may also occur here.
SUBDURAL SPACE
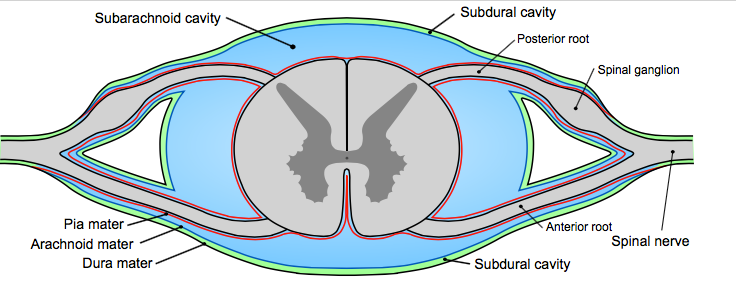
The subdural space (or subdural cavity) is a potential space that can be opened by the separation of the arachnoid mater from the dura mater as the result of trauma, pathologic process, or the absence of cerebrospinal fluid as seen in a cadaver. In the cadaver, due to the absence of cerebrospinal fluid in the subarachnoid space, the arachnoid mater falls away from the dura mater. It may also be the site of trauma, such as a subdural hematoma, causing abnormal separation of dura and arachnoid mater. Hence, the subdural space is referred to as "potential" or "artificial" space.
SUBARACHNOID SPACE
In the central nervous system, the subarachnoid space (subarachnoid cavity) is the anatomic spacebetween the arachnoid mater and the pia mater.
in which the cerebrospinal fluid is contained.
In the spine, the epidural space (from Ancient Greek ἐπί, "on, upon" + dura mater also known as "epidural cavity", "extradural space" or "peridural space") is an anatomic space that is the outermost part of the spinal canal.
In humans the epidural space contains lymphatics, spinal nerve roots, loose connective tissue, fatty tissue, small arteries, and a network of internal vertebral venous plexuses.
In humans[edit]The upper limit of the epidural space is the foramen magnum, which is the point where the spine meets the base of the skull. The lower limit is at the tip of the sacrum, at the sacrococcygeal membrane.
In the head, the epidural space is known as a potential space. In rare circumstances, a torn artery (e.g. the middle meningeal artery) may cause bleeding which is sufficient to create epidural space; this is an epidural hematoma.
The space between the dura and the arachnoid (in both head and spine), the subdural space, is also a potential space. Bleeding may also occur here.
SUBDURAL SPACE
The subdural space (or subdural cavity) is a potential space that can be opened by the separation of the arachnoid mater from the dura mater as the result of trauma, pathologic process, or the absence of cerebrospinal fluid as seen in a cadaver. In the cadaver, due to the absence of cerebrospinal fluid in the subarachnoid space, the arachnoid mater falls away from the dura mater. It may also be the site of trauma, such as a subdural hematoma, causing abnormal separation of dura and arachnoid mater. Hence, the subdural space is referred to as "potential" or "artificial" space.
SUBARACHNOID SPACE
In the central nervous system, the subarachnoid space (subarachnoid cavity) is the anatomic spacebetween the arachnoid mater and the pia mater.
in which the cerebrospinal fluid is contained.
These images are in Public Domain - No Copyrights-

A lumbar puncture (or LP, and colloquially known as a spinal tap) is a medical procedure in which a needle is inserted into the spine, most commonly to collect cerebrospinal fluid (CSF) for diagnostic testing-
is used to access the subarachnoid space and fluid collected-
It is regarded as a safe procedure, but post-dural-puncture headache is common.
Therapeutic[edit]Lumbar punctures may also be done to inject medications into the cerebrospinal fluid ("intrathecally"), particularly for spinal anesthesia[6] or chemotherapy.
Spinal anaesthesia (or spinal anesthesia), also called spinal analgesia[citation needed], spinal block or subarachnoid block (SAB), is a form of regional anaesthesia involving injection of a local anaesthetic into the subarachnoid space, generally through a fine needle, usually 9 cm long (3.5 inches).
Medical uses[edit]Spinal anaesthesia is a commonly used anaesthetic technique, both alone and in combination with either sedation or general anaesthesia. Examples of uses include :-
Limitations[edit]Spinal anaesthetics are typically limited to procedures involving most structures below the upper abdomen. To administer a spinal anaesthetic to higher levels may affect the ability to breathe by paralysing the intercostal respiratory muscles, or even the diaphragm in extreme cases (called a "high spinal", or a "total spinal", with which consciousness is lost), as well as the body's ability to control the heart rate via the cardiac accelerator fibres. Also, injection of spinal anaesthesia higher than the level of L1 can cause damage to the spinal cord, and is therefore usually not done.
Difference from epidural anesthesia[edit]
Schematic drawing showing the principles of spinal anesthesia.Epidural anesthesia is a technique whereby a local anesthetic drug is injected through a catheter placed into the epidural space. This technique has some similarity to spinal anesthesia, both are neuraxial, and the two techniques may be easily confused with each other. Differences include:
is used to access the subarachnoid space and fluid collected-
It is regarded as a safe procedure, but post-dural-puncture headache is common.
Therapeutic[edit]Lumbar punctures may also be done to inject medications into the cerebrospinal fluid ("intrathecally"), particularly for spinal anesthesia[6] or chemotherapy.
Spinal anaesthesia (or spinal anesthesia), also called spinal analgesia[citation needed], spinal block or subarachnoid block (SAB), is a form of regional anaesthesia involving injection of a local anaesthetic into the subarachnoid space, generally through a fine needle, usually 9 cm long (3.5 inches).
Medical uses[edit]Spinal anaesthesia is a commonly used anaesthetic technique, both alone and in combination with either sedation or general anaesthesia. Examples of uses include :-
- Orthopaedic surgery on the pelvis, femur, tibia and the ankle
- Hip replacement
- Knee replacement
- Hip fracture surgery
- Spinal opioids e.g. Diamorphine 500-1000mcg along with general anaesthesia for post operative analgesia in laparoscopic bowel surgery
- Lower limb vascular surgery
- Endovascular aortic aneurysm repair
- Hernia (inguinal or epigastric)
- Haemorrhoidectomy (Piles), fistulae and fissures
- Nephrectomy and Cystectomy in combination with general anaesthesia
- Transurethral resection of the prostate and transurethral resection of bladder tumours
- Abdominal and vaginal hysterectomies
- Laparoscopy assisted vaginal hysterectomies combined with general anaesthesia
- Caesarean sections
- Non-availability of patient's consent
- Local infection or sepsis at the site of lumbar puncture
- Bleeding disorders, thrombocytopaenia, or systemic anticoagulation (secondary to an increased risk of a spinal epidural hematoma)
- Space occupying lesions of the brain
- Anatomical disorders of the spine
- Hypovolaemia e.g. following massive haemorrhage, including in obstetric patients
- Hypotension (Spinal shock) - Due to sympathetic nervous system blockade. Common but usually easily treated with intravenous fluid and sympathomimmetic drugs such as Ephedrine, Phenylephrine or Metaraminol
- Post dural puncture head ache (PDPH) or post spinal head ache - Associated with the size and type of spinal needle used
- Cauda equina injury - very rare, due to the insertion site being too high
- Cardiac arrest - very rare, usually related to the underlying medical condition of the patient
- Spinal canal haematoma, with or without subsequent neurological sequelae due to compression of the spinal nerves. Urgent CT/MRI to confirm the diagnosis followed by urgent surgical decompression to avoid permanent neurological damage
- Epidural abscess, again with potential permanent neurological damage. May present as meningitis or and abscess with back pain, fever, lower limb neurological impairment and loss of bladder/bowel function. Urgent CT/MRI confirms the diagnosis followed by antibiotics and urgent surgical drainage
Limitations[edit]Spinal anaesthetics are typically limited to procedures involving most structures below the upper abdomen. To administer a spinal anaesthetic to higher levels may affect the ability to breathe by paralysing the intercostal respiratory muscles, or even the diaphragm in extreme cases (called a "high spinal", or a "total spinal", with which consciousness is lost), as well as the body's ability to control the heart rate via the cardiac accelerator fibres. Also, injection of spinal anaesthesia higher than the level of L1 can cause damage to the spinal cord, and is therefore usually not done.
Difference from epidural anesthesia[edit]
Schematic drawing showing the principles of spinal anesthesia.Epidural anesthesia is a technique whereby a local anesthetic drug is injected through a catheter placed into the epidural space. This technique has some similarity to spinal anesthesia, both are neuraxial, and the two techniques may be easily confused with each other. Differences include:
- The injected dose for an epidural is larger, being about 10–20 mL compared to 1.5–3.5 mL in a spinal.
- In an epidural, an indwelling catheter may be placed that serves for additional injections, while a spinal is almost always a one-shot only.
- The onset of analgesia is approximately 25–30 minutes in an epidural, while it is approximately 5 minutes in a spinal.
- An epidural often does not cause as significant a neuromuscular block as a spinal, unless specific local anesthetics are also used which block motor fibres as readily as sensory nerve fibres.
- An epidural may be given at a cervical, thoracic, or lumbar site, while a spinal must be injected below L2 to avoid piercing the spinal cord.
- CC BY-SA 3.0view terms
- File:Prinzip der Spinalanaesthesie.png
- Uploaded by PhilippN
- Created: Spring 2007
 RSS Feed
RSS Feed
